
A concussion refers to a form of traumatic brain injury that causes a disturbance of the brain’s normal functioning but that does not result in any structural change to the brain. This disturbance of mental functioning can result in a broad spectrum of symptoms and signs such as headache, dizziness, poor sleep, balance disturbances, poor concentration and memory loss. These negative alterations of mental functioning are important in cycling because of the risk to the individual of a repeated crash should they return to training or competition earlier than advised.
Concussions occur by far the commonest in rugby and other contact sports. As a result of the high incidence of concussions in these sports, a clinical assessment tool called the SCAT5 (Sports Concussion Assessment Tool) was developed for the diagnosis of concussion in sport. A full PDF of the tool is available through the British Journal of Sports Medicine here.
scat5 assessment

The SCAT5 contains two sections: an immediate assessment and a delayed assessment. The immediate assessment is normally carried out on the side of the field at the time of the incident and is intended to identify obvious immediate signs and symptoms of a concussion, such as a loss of consciousness, vomiting or disorientation. An athlete that is displays any of these signs is withdrawn from play immediately, diagnosed with a concussion, and the delayed assessment is then carried out away from the field (e.g. in the medical area). The delayed assessment is a more comprehensive examination that looks for clues that suggest a disturbance of mental functioning such as short-term memory loss, problems concentrating and a balance disturbance.
The SCAT5 is a tool that is well adapted to use in field sports where there is provision for an athlete to be removed from play or for the game to be paused in order to carry out an appropriate assessment. But what does one do in cycling where there is no provision to withdraw a rider in order to perform an evaluation of them?
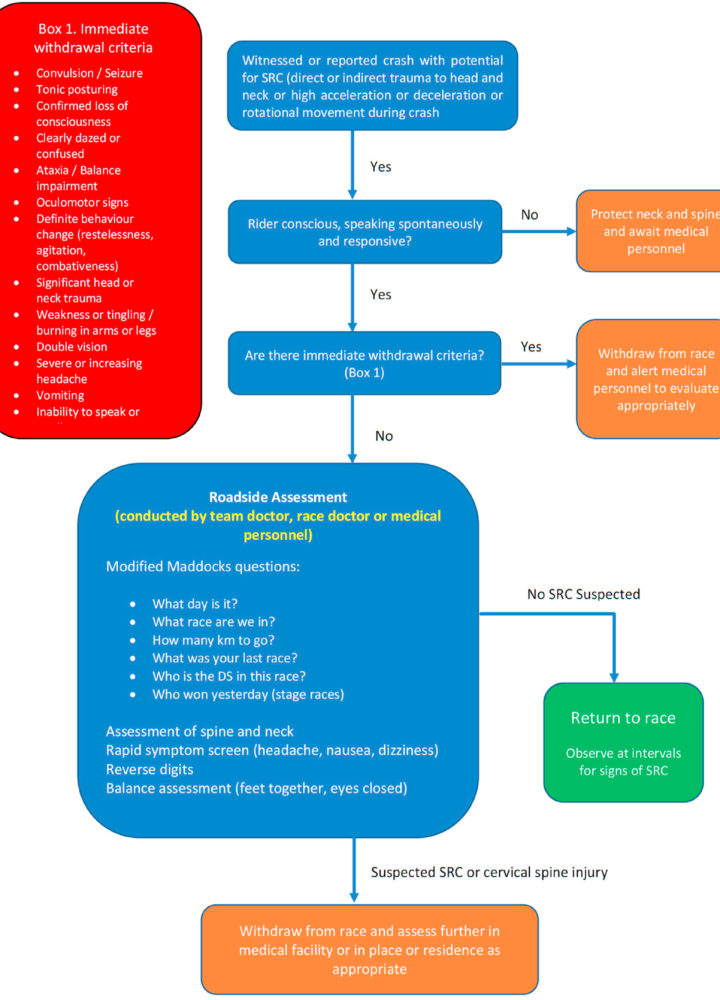
HARROGATE CONSENSUS FOR UCI
To try and answer this question, the Harrogate consensus was proposed by a collection of experts on behalf of the UCI in 2021. This document (the full version of which can be accessed here) lays out a suggested algorithm specific to cycling that might allow for a faster and more appropriate assessment of a cyclist following a crash during a competitive event. An image of this pathway is contained within the full document.
After a concussion, a return to full training and competition, is separated into two steps:
- Return to work; followed by
- Return to sport
Each of these two steps is carried out in a stepwise fashion, the full details of which can be found in the SCAT5. The important point is that, before an individual attempts to resume training, they must be able to tolerate a full day’s worth of mental strain (i.e. a day at work) without experiencing any symptoms related to their concussion. Exercise is a far greater physiological challenge than a day at work and should therefore only be attempted following the proven tolerance of a normal day’s mental strain.
return to training and competition
From a practical perspective, a typical return to full training would consist of an initial period of 24 hours of full mental and physical rest, followed by 7 days of rest from exercise during which the individual would ideally conduct a graded return to work or school. The process of returning to training can then move forwards. In a contact sport, this is done by first adding light exercise and then slowly adding activity up to full contact practice and ultimately competition. In cycling, the stages of returning to full training are instead separated on the basis of intensity. All training is initially done indoors until the cyclist is able to tolerate high-intensity intervals without any exacerbation of symptoms, after which they may return to riding outdoors.
To try and answer this question, the Harrogate consensus was proposed by a collection of experts on behalf of the UCI in 2021. This document (the full version of which can be accessed here) lays out a suggested algorithm specific to cycling that might allow for a faster and more appropriate assessment of a cyclist following a crash during a competitive event. An image of this pathway is contained within the full document.
The Harrogate Consensus also outlines a suggested return to play similar to the one discussed in this article but the further discussion of which is beyond the scope of this article.
A PROPOSED PROGRESSION MAY LOOK LIKE THIS
1) COMPLETE REST – 24 hours
- 2) INITIAL REST – full 7 days, symptom-tolerated activity (e.g. walking); ideally used to return to work/school
- 3) LIGHT AEROBIC ACTIVITY – only once returned to work/school; two steps
- 1) Zone 1 – 24 hours; e.g. 1 hour (Z1 only)
- 2) Zone 2 – 24 hours; e.g 1h15 (do not exceed Z2)
- 4) ADD INTENSITY
- 1) Zone 2 + Zone 3 – 24 hours; e.g. 2x 15:00 (Z3)
- 2) Zone 3 + Zone 4 – 24 hours; e.g. 2x 15:00 in Z3 w/ second half in Z4
- 3) Zones 3,4 + 5 – 24 hours; e.g. 8:00 (Z3) 5:00 (Z4) 2:00 (Z5)
- 5) STRUCTURED WORKOUT (partial)
- Includes both mental and physical challenge. (Requires concentration as well as heavy physical exertion.)
- 6) STRUCURED WORKOUT (full)
- Further mental and physical strain.
- 7) RETURN TO COMPETITION
A progression such as this would typically take around 2 weeks to complete but may end up taking longer. This is because an athlete cannot be allowed to progress from one step to the next unless they have been able to tolerate the current step without any exacerbation of symptoms. In the event that a particular step exacerbates symptoms (e.g. a headache during or after exercise), the athlete should move back one step and complete the preceding stage again before attempting the un-tolerated stage once more. It is important to be flexible and to recognise that the process of recovery is seldom linear and will often require several steps backwards before the athlete returns to competition.
In summary, a concussion results in a disturbance of mental functioning that necessitates the immediate removal of a cyclist from racing. A unique challenge related to concussions in cycling is the difficulty of assessing the rider without provision for them to be temporarily removed from play. A graduated return to work and then training is of paramount importance and should be carried out in a stepwise fashion. A return to training should only begin once a normal day’s worth of mental strain is tolerated without complaint.
Appreciation of the marked disruption that concussion creates in mental functioning and strict adherence to the graduated return to training is likely to result in an earlier return to competition than if the process is not fully respected or rushed. The assessment and further management of an individual with a concussion should always be carried out under the guidance of an appropriate medical professional.
DISCLAIMER: this website does not provide medical adviCe
The information, including but not limited to, text, graphics, images and other material contained on this website are for informational purposes only. No material on this site is intended to be a substitute for professional medical advice, diagnosis or treatment. Always seek the advice of your physician or other qualified health care provider with any questions you may have regarding a medical condition or treatment and before undertaking a new health care regimen, and never disregard professional medical advice or delay in seeking it because of something you have read on this website.